Atrial Septal Defect - Surgery
An atrial septal defect (ASD) is a hole in the atrial septum, the upper wall of the heart separating the right and left atria. Surgery is occasionally necessary to close an atrial septal defect in a child. This most commonly occurs in the setting of a large or moderate size hole. The most common indication for surgery is the presence of dilation of heart chambers, specifically the right ventricle, due to long-standing excess blood flow. Typically surgery is performed between 2 and 5 years of age, although it can easily be accomplished earlier if necessary.
History
The first successful open heart surgery to close an atrial septal defect was performed in 1952 by John Lewis and associates at the University of Minnesota. This was actually the first of successful open heart procedure of any type and marked beginning of the open heart surgery era. Since that time, surgical techniques and progress have improved tremendously. In this day and age, surgical closure of an ASD in children is generally considered a safe operation.
ASD Surgery
Because the hole created by an atrial septal defect is inside the heart, the heart must be drained of blood prior to any operation or manipulation. This requires the use of cardiopulmonary bypass. Cardiopulmonary bypass refers to the technique by which blood is diverted from the heart and lungs by a machine that subsequently removes carbon dioxide and supplies oxygen. Oxygenated blood is returned from the machine to the aorta. With the heart empty of blood, the surgeon is then able to safely open it, find the hole, and patch it closed.
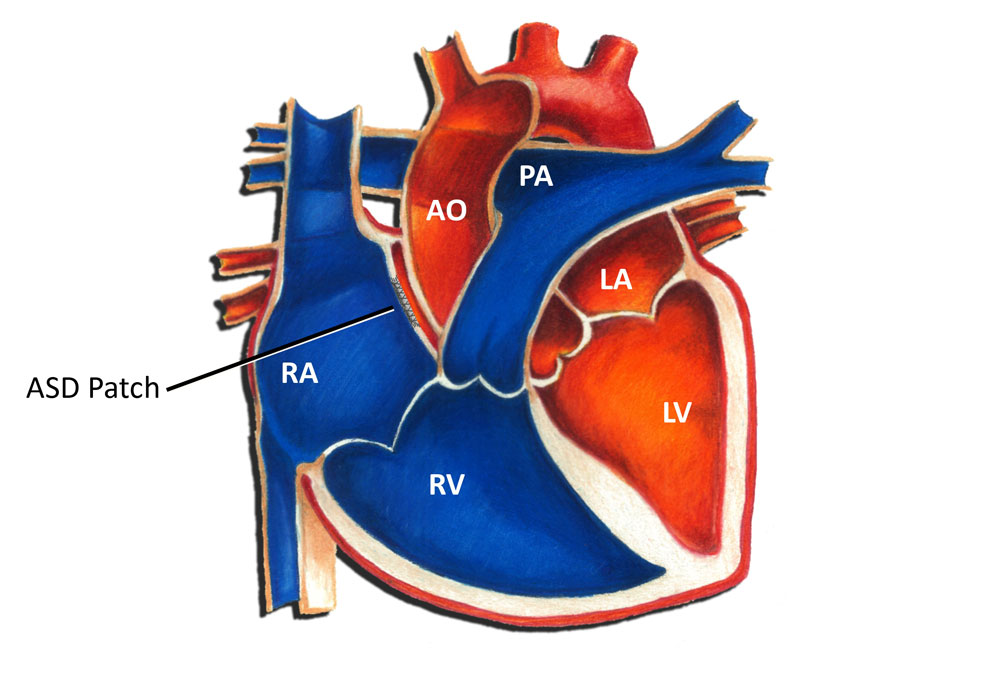 Typically the patch used to close an ASD is made from a piece of pericardium, the sac which normally covers the heart. This avoids the use of any synthetic or foreign material. The surgeon uses suture material to stitch the pericardial patch into place. In some instances the surgeon is able to close the hole without a patch by simply drawing the edges together. Usually closing an ASD is relatively straightforward. Once the patch is sutured into place and the hole is closed, the patient is removed from cardiopulmonary bypass. Blood returns to the heart and the operation is complete at this point.
Typically the patch used to close an ASD is made from a piece of pericardium, the sac which normally covers the heart. This avoids the use of any synthetic or foreign material. The surgeon uses suture material to stitch the pericardial patch into place. In some instances the surgeon is able to close the hole without a patch by simply drawing the edges together. Usually closing an ASD is relatively straightforward. Once the patch is sutured into place and the hole is closed, the patient is removed from cardiopulmonary bypass. Blood returns to the heart and the operation is complete at this point.
Occasionally other heart defects may be found in association with an atrial septal defect. For example, a ventricular septal defect, a patent ductus arteriosus, or pulmonary valve stenosis may all potentially complicate the surgery. Fortunately, addressing these defects as well typically does not increase the complexity of the surgery significantly.
Fortunately over time the natural tissue of the heart grows over the ASD patch and seals it into place. Usually this process takes about 6-12 months. Because of this, the patch never has to be replaced or removed as a child grows. Once an ASD is closed, it is typically closed for good!
Atrial septal defect device closure is a relatively recent procedure that is an alternative to traditional surgery. In general, this is a very safe procedure that offers an excellent option to certain children who meet criteria regarding the size and position of the hole.
Outcomes
The outcome for most children who undergo atrial septal defect surgery is excellent. The usual hospital stay is 2-4 days. Most children are able to return to full activity within several weeks. All children who undergo heart surgery are required to take antibiotics before any dental or surgical procedures for at least 6 months following surgery (SBE prophylaxis). The manipulation of the heart and the presence of suture material in the heart increases the risk of infection at any time bacteria may enter the bloodstream. This can happen with dental work and certain forms of surgery. After 6 months, usually the normal heart tissue has sealed things in place sufficiently to no longer require this.
The vast majority of children who undergo atrial septal defect surgery do very well long-term. For most this is the only surgery they will ever require! Most children are able to return to full activity within several weeks. The long-term prognosis for a child who has had an atrial septal defect repaired surgically is excellent.