Coarctation of the Aorta - Surgery
A coarctation of the aorta is a narrowing of the aorta that results in the heart having to squeeze harder to force blood past the narrowed area. Most patients with coarctation of the aorta require surgery to correct the condition. Often children are diagnosed as newborn infants; in this setting they frequently have symptoms and occasionally may be critically ill. When patients are diagnosed as older children they frequently come to attention because of long-standing high blood pressure.
History
The first successful repair of coarctation of the aorta was performed by Dr. Clarence Crafoord in 1944. However, it wasn't until the mid 1970s to early 1980s that successful repair of more significant coarctation of the aorta in babies in infants was able to be performed. Over the years surgical techniques have advanced to allow for even the most complicated coarctation repairs to be done with good outcomes.
Coarctation Surgery
Surgery for coarctation of the aorta is typically done through a thoracotomy. A thoracotomy is an incision on the upper left side of the back. Because the aorta actually dives back in the body as it turns to the carry blood downwards, a coarctation is usually more easily accessed from this approach, as opposed to from the front of the chest. Occasionally it may be necessary to fix a coarctation from the front of the chest if there is a long segment of narrowing involved.
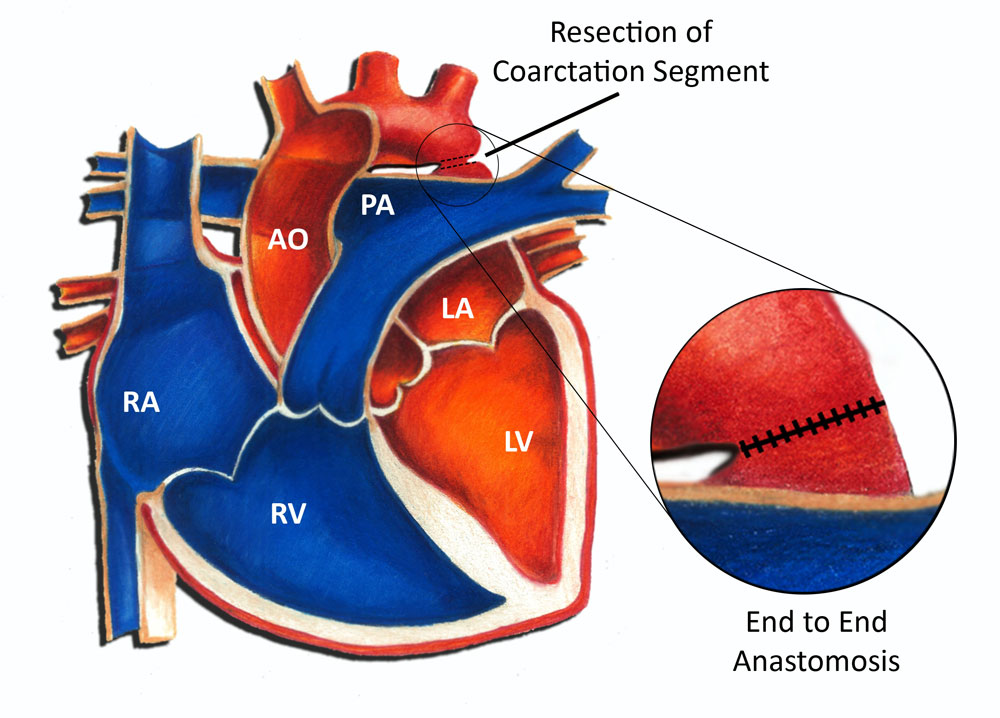 With a thoracotomy, the surgeon spreads the ribs and moves the lung out of the way. Because the aorta is outside the heart, cardiopulmonary bypass is not necessary. After locating the coarctation, the surgeon transiently occludes blood flow above and below the area of narrowing. With blood flow occluded, the surgeon removes the narrowed area and then sutures the remaining two ends together, as shown in the diagram above. This procedure is called an end to end anastomosis.
With a thoracotomy, the surgeon spreads the ribs and moves the lung out of the way. Because the aorta is outside the heart, cardiopulmonary bypass is not necessary. After locating the coarctation, the surgeon transiently occludes blood flow above and below the area of narrowing. With blood flow occluded, the surgeon removes the narrowed area and then sutures the remaining two ends together, as shown in the diagram above. This procedure is called an end to end anastomosis.
Outcomes
The vast majority of patients who undergo surgical repair of a coarctation do very well. Most older children spend anywhere from 2-4 days in the hospital after surgery. Usually they are cleared to return to full activity within 6 weeks. Babies and infants with more complicated coarctation and aortic arch abnormalities may require a much longer hospital stay. All patients who undergo coarctation surgery are required to take antibiotics before any dental or surgical procedures for 6 months following the procedure (SBE prophylaxis).
In summary, surgery for coarctation of the aorta in this day and age is generally a safe and effective procedure. The vast majority of children who undergo this surgery do very well long-term.